Majid Haghjoo, Arash Arya, Mohammadreza Dehghani, Zahra Emkanjoo, 68
Amirfarjam Fazelifar, MohammadAli Sadr-Ameli., “Multiple Arrhythmogenic
Substrate for Tachycardia in a Patient with Frequent Palpitations”
fibrillation and; 3) patients with Ebstein anomaly.9
Dual AV nodal physiology is known to occur in 8-40% of patients with AP, leading to a
variety of possible reentrant circuits.10,11 In the study of Csanadi Z et al.12, the most common
arrhythmia in these patients were AVRT without AVNRT (75%), whereas 19% of patients had
both AVRT and AVNRT, and 6% had only AVNRT. They also demonstrated that absence of
clinical tachycardia during follow up in those with only dual AV nodal physiology with or
without single echo cycle would argue against the routine ablation of the SP in these patients. At
times, one tachycardia changes into another as depicted in an interesting case report.13
Click here to enlarge
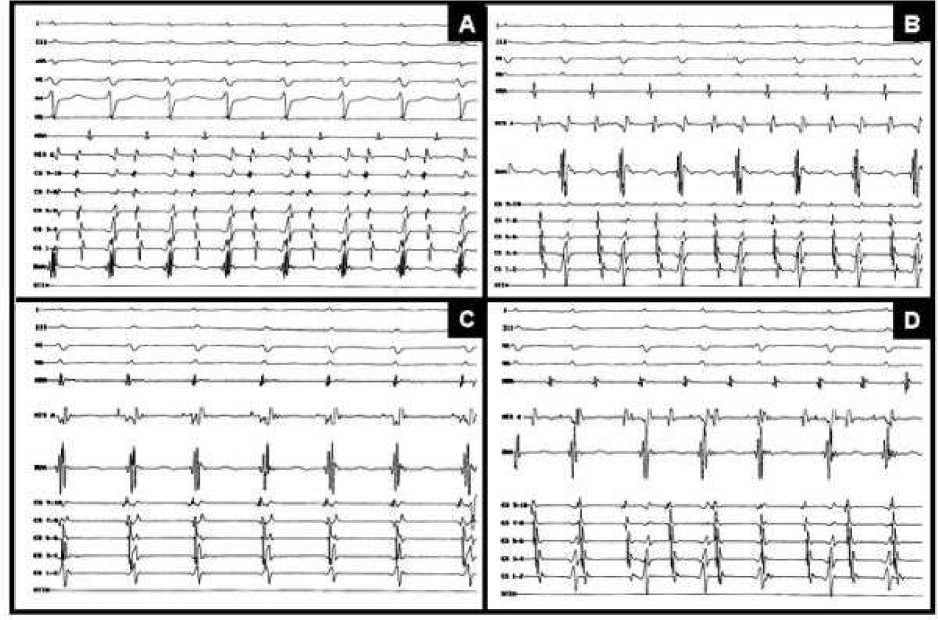
Figure 1. Four different types of SVTs induced during EPS. A, a narrow complex
tachycardia (CL=320 ms) with earliest atrial activity in CS 9-10, compatible with
AVRT using bypass tract as retrograde limb of tachycardia. B, another narrow
complex tachycardia (CL=340 ms) induced after ablation of RPS-AP. Note that
earliest atrial activity was recorded in HRA catheter, compatible with RFW-AP. C,
typical AVNRT (CL=360 ms) induced after ablation of both right-sided APs. D,
self-terminating AT induced after SP ablation.
SVT= supraventricular tachycardia; EPS =electrophysiologic study; CL= cycle
length; AVRT=atrioventricular reentrant tachycardia; AVNRT=atrioventricular
nodal reentrant tachycardia; RPS-AP=right posteroseptal accessory pathway;
HRA=high right atrium; RFW-AP=right free-wall accessory pathway; AT=atrial
tachycardia; SP=slow pathway; HIS=His recording catheter; RVA=right
ventricular apex.
Indian Pacing and Electrophysiology Journal (ISSN 0972-6292), 5(1): 66-70 (2005)
More intriguing information
1. The name is absent2. The name is absent
3. Fiscal Rules, Fiscal Institutions, and Fiscal Performance
4. A Duality Approach to Testing the Economic Behaviour of Dairy-Marketing Co-operatives: The Case of Ireland
5. Qualifying Recital: Lisa Carol Hardaway, flute
6. The name is absent
7. The name is absent
8. Population ageing, taxation, pensions and health costs, CHERE Working Paper 2007/10
9. Implementation of a 3GPP LTE Turbo Decoder Accelerator on GPU
10. The name is absent