Onfvie JvunieifσfHeeift fι anefββιeefSciences
Introduction:
Hydatid disease is a parasitic infection caused by the larval
stage of the cestode, Echinococcus granulosus. It is endem-
ic in many parts of the world, including India. Most fre-
quently it affects the liver and lung. Involvement of the
peritoneal cavity is uncommon, accounting for 13% of ab-
dominal echinococcosis. Unusual locations as well as multi-
ple primary or secondary hydatid disease pose special ther-
apeutic challenges.(1) We report a case of disseminated
abdominal hydatosis who presented with features of ob-
structive uropathy and investigations revealed hydatid cyst
in rectovesical pouch besides liver, spleen and peritoneum.
Case Report:
A 28 year male shepherd presented with a dull aching pain
and gradually increasing lump in the right hypochondrium
and epigastric region over six months. There was history of
acute retention of urine thrice in the past twelve days for
which patient was catheterized. Anorexia and weight loss
were associated complaints. History of constipation was
also present. There was no history of jaundice. He was op-
erated upon for hepatic hydatic disease seven years back.
Examination revealed multiple cystic swellings in abdomen.
Hepatospleenomegally was present. Both liver and spleen
were having irregular surface with multiple, nontender cys-
tic masses palpable over the surface. Soft irregular masses
were also felt in the umbilical and hypogastric regions. On
per rectal examination, a mass was felt from anterior rectal
wall but rectal mucosa was free. Review of other systems
was normal. On laboratory investigations hemogram re-
vealed mild increase in the eosinophil count (3%) and
raised ESR (55mm at the end of 1 hour) , Biochemistry
screen revealed normal investigations including a normal
liver function profile. Test for antibodies against
Echinococcus granulosus was 15.99 U/ml and was positive.
Ultrasound examination of the abdomen and pelvis re-
vealed multiple, thin walled cystic lesions of variable size in
the liver and spleen with cartwheel appearance. The peri-
toneum and the pelvis were studded with similar cystic le-
sions. Plain CT scan of the abdomen revealed multiple, well
defined cystic lesions throughout the abdomen.(Fig-1) The
cysts were multi loculated with multiple internal septations
suggestive of hydatid disease. Liver and spleen appear to
be replaced by the multiseptated cysts.(Fig-2) A large cyst
is seen in the pelvic cavity producing a pressure affect on
surrounding structures but not invading them.(Fig-3) A di-
agnosis of secondary echinococcosis was made on clinical
features and investigations. Patient was started on albenda-
zole (15mg/kg/day) and follow up was advised. Patient has
been lost in the follow up.
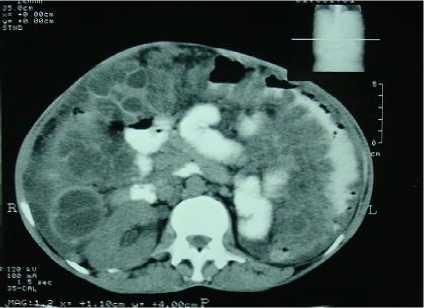
Figure-1 CT abdomen showing peritoneal hydatid cyst

Figure-2 CT abdomen showing hydatid cyst in liver and
spleen

Figure-3 CT abdomen showing hydatid cyst in rec-
tovesical pouch
OJHAS Vol 7 Issue 2(10) Raina S et al Giant intra-abdominal hydatid cysts with multivisceral locations.
http://ojhas.org
More intriguing information
1. Road pricing and (re)location decisions households2. Cultural Neuroeconomics of Intertemporal Choice
3. Barriers and Limitations in the Development of Industrial Innovation in the Region
4. The name is absent
5. Willingness-to-Pay for Energy Conservation and Free-Ridership on Subsidization – Evidence from Germany
6. Clinical Teaching and OSCE in Pediatrics
7. The name is absent
8. Better policy analysis with better data. Constructing a Social Accounting Matrix from the European System of National Accounts.
9. Uncertain Productivity Growth and the Choice between FDI and Export
10. The name is absent