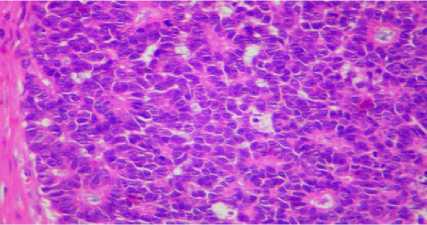
Figure 2: Photomicrograph showing Homer-wright rosettes
(H&E X 400)
Discussion:
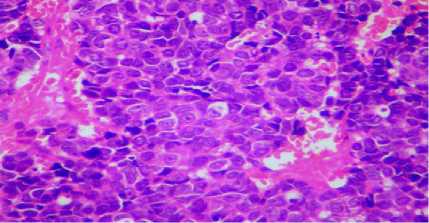
Figure 3: Photomicrograph showing tumor cells with vesi-
cular nucleus with nucleoli & moderate amount of cyto-
plasm (H&E X 400)
IHC was strongly positive for NSE, CK cocktail and S-100. S-
100 showed positivity of sustentacular cells along the periphery
of the tumor lobules with few cells within the tumor Lobules
(Fig 4 & 5).
Figure 4: Photomicrograph of immunohistochemical stain-
ing showing S-100 positivity of the sustentacular cells in the
as well as within the lobiules (X 400)
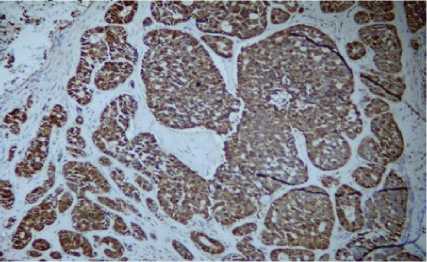
Figure 5: Photomicrograph of immunohistochemical stain-
ing of the tumor cells showing Non Specific Esterase positiv-
ity (X 400)
The final diagnosis of olfactory neuroblastoma grade IV was
made.
Debulking surgery was done.The patient had an uneventful post
operative period and was subjected for radiotherapy.
Olfactory neuroblastoma is an uncommon malignant neoplasm,
representing 2-3% of sinonasal tract tumors with an incidence
of approximately 6 %.1,2 These tumors arise from the olfactory
neuro epithelium, which extends from the roof of the nose to
the area of the superior turbinate and a portion of the nasal
septum.2
There is no gender predilection;1 some authors report a male to
female ratio of 2:1.3 It occurs in all age groups with a bimodal
peak in the 2nd and 6th decade.4
The usual clinical symptoms are unilateral nasal obstruction,
epistaxsis, anosmia, headache, pain and ocular disturbances. 1
ONB has a tendency to spread sub mucosally to involve the
paranasal sinuses, nasal cavity and other structures like oral
cavity, orbits and the brain.3
Olfactory neuroblastoma of grade I & II (Hyams grade) can be
easily recognized as they resemble other neuroblastomas with
small round cells arranged in rosettes and an abundant neuro
fibrillary background.1 Grade III & IV (Hyams grade) have
little or no neuro fibrillary background with few or no rosette
formations making morphological diagnosis difficult. In our
case, some of the cells had an epithelial appearance with vesi-
cular nucleus and comedo necrosis closely resembling undiffer-
entiated sinonasal carcinoma. The other differential diagnosis
of small cell neuroendocrine carcinoma was considered as the
tumor cells showed rosette arrangement with absent neuro fib-
rillary background. Some areas showed cribriform pattern
which is known to occur in ONB and neuroendocrine car-
cinoma favoring differentiation rather than existence of two
separate neoplasms.4 With confounding histomorphology, the
diagnosis will be difficult which requires immunohistochem-
istry for confirmation.
ONB shows variable positivity for Cyto keratin, synaptophysin
and chromogranin. One of the studies showed cytokeratin
(4/11), synaptophysin (7/11) and chromogranin A (1/11).5
The main mode of treatment is complete craniofacial resection
of the tumor followed by radiotherapy. 6 The prognosis depends
on the grade and stage of the tumor. The 5 year survival Rate is
40% for high grade tumors with a high local recurrence (15-
70%).1
Conclusion:
Olfactory neuroblastoma is an uncommon neoplasm of the
sinonasal tract. Histologically, the tumor can have varied cyto-
morphological appearance with absence of neurofibrillary mat-
rix and occasional areas with rosette formation. IHC will be of
immense help in differentiating it from the undifferentiated
sinonasal carcinoma.
References:
1. Christopher DM Fletcher. Tumors of the upper respiratory
tract. In Christopher DM Fletcher. Diagnostic histopatho-
logy of tumors. 3rd ed. Elsevier, 2007. pp 112-118.
2. Ghaffar, Shehzad, Salahuddin, et al. Olfactory neuro-
blastoma: a case report and review of the literature. Ear,
Nose and Throat Journal. 2005 March;84(3):150-52.
3. Arafat Ayoub, Mohammed Ali Hiari. Olfactory neuro-
blastoma: A Case Report. Journal of Research in Medical
Sciences. Dec 2005;12(2):48-50.
4. Roasi J. Respiratory tract. In Rosai J, ed Ackerman’s Sur-
gical Pathology. 9th ed. Elsevier 2004;Vol 1. pp 316-17.
5. Frierson HF Jr, Ross GW, Mills SE,et al. Olfactory neuro-
blastoma. Additional immunohistochemical characteriza-
tion. Am J Clin pathol. 1991 Jun;95(6):903.
6. Mills, Stacey EMD, Frierson, et al. Olfactory neuro-
blastoma: A clinicopathologic study of 21 cases. The Am J
of Surg Pathol 1995;9:317-327.
More intriguing information
1. Economie de l’entrepreneur faits et théories (The economics of entrepreneur facts and theories)2. he Virtual Playground: an Educational Virtual Reality Environment for Evaluating Interactivity and Conceptual Learning
3. Poverty transition through targeted programme: the case of Bangladesh Poultry Model
4. The name is absent
5. The name is absent
6. National curriculum assessment: how to make it better
7. The constitution and evolution of the stars
8. A Dynamic Model of Conflict and Cooperation
9. AN ANALYTICAL METHOD TO CALCULATE THE ERGODIC AND DIFFERENCE MATRICES OF THE DISCOUNTED MARKOV DECISION PROCESSES
10. Activation of s28-dependent transcription in Escherichia coli by the cyclic AMP receptor protein requires an unusual promoter organization