precisely the factors that should most strongly predict a negative affective response to the child
rearing endeavor, and in fact they do (although a prior history of depression, question seven, is
a strong predictor of PPD, this factor is neutral with respect to the defection hypothesis and will
not be addressed in this paper).

Prepartum questions:
1. Are you single or separated?
2. Do you have marital problems?
3. Do you often feel that your husband
(boyfriend) does not love you?
4. Was your pregnancy unplanned
(accidental)?
5. Do you more or less regret that you
are pregnant?
6. Can you honestly say at this time that
you really do not desire to have a
child?
7. Did you become very depressed or
extremely nervous in the period
following the birth of your last child?
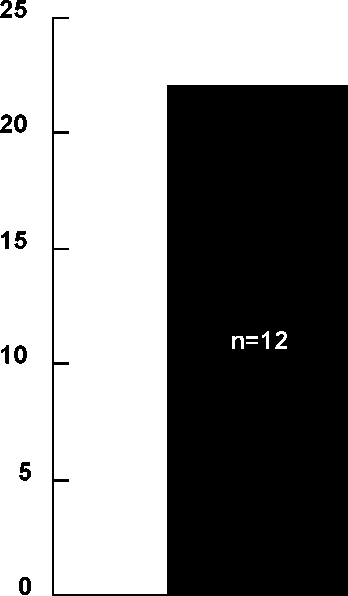
n=12
Answered yes to at least
three prepartum questions
Answered no to all seven
prepartum questions
Figure 1: Prepartum factors that predict postpartum depression (data from Field, et al. 1985).
In summary, women without social support, particularly the father’s support, are at
significantly increased risk for PPD.
Prediction 2: Low infant viability should predict negative affect
Problems with the baby decrease the mother’s fitness benefits (on average), and should
therefore increase the odds that she will experience negative affect postpartum. As noted
above, pregnancy and delivery problems are significant predictors of child morbidity and
mortality, and should therefore also predict negative affect postpartum. Consistent with these
predictions, a number of studies show strong correlations in the expected direction between
pregnancy, delivery, and infant problem variables and PPD (table 2)3. As with social support,
3Haig (1993) argues that gestational diabetes and pregnancy induced hyptertension, two important types of
pregnancy problems, are fetal strategies to extract additional resources from the mother when circumstances
indicate that the father is less likely to invest. If so, their association with PPD may be through the shared variable
of social support rather than their association with higher rates of perinatal morbidity and mortality, and therefore
cannot be construed as evidence in favor of the defection hypothesis. An alternate hypothesis is that the fetus may
13
More intriguing information
1. Bargaining Power and Equilibrium Consumption2. EDUCATIONAL ACTIVITIES IN TENNESSEE ON WATER USE AND CONTROL - AGRICULTURAL PHASES
3. Evolving robust and specialized car racing skills
4. La mobilité de la main-d'œuvre en Europe : le rôle des caractéristiques individuelles et de l'hétérogénéité entre pays
5. The name is absent
6. Inflation Targeting and Nonlinear Policy Rules: The Case of Asymmetric Preferences (new title: The Fed's monetary policy rule and U.S. inflation: The case of asymmetric preferences)
7. NATURAL RESOURCE SUPPLY CONSTRAINTS AND REGIONAL ECONOMIC ANALYSIS: A COMPUTABLE GENERAL EQUILIBRIUM APPROACH
8. The name is absent
9. The name is absent
10. Rural-Urban Economic Disparities among China’s Elderly