Fletcher et al. BMC Cardiovascular Disorders 2010, 10:37
http://www.biomedcentral.com/1471-2261/10/37
Page 5 of 8
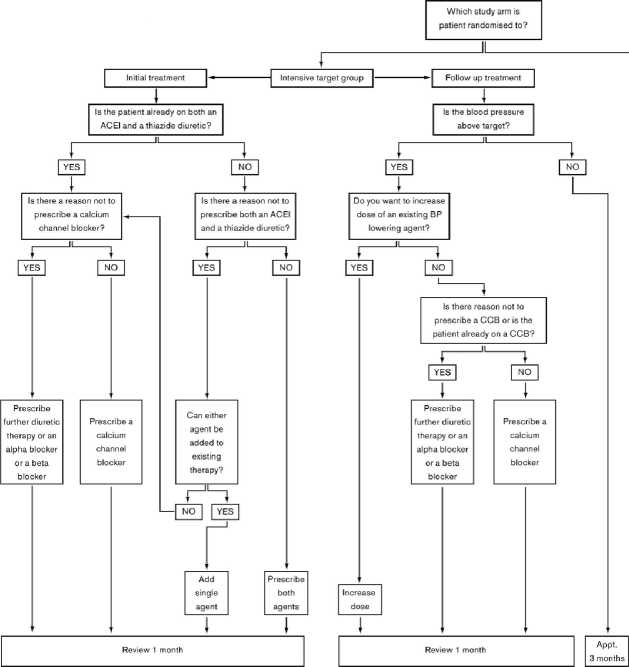
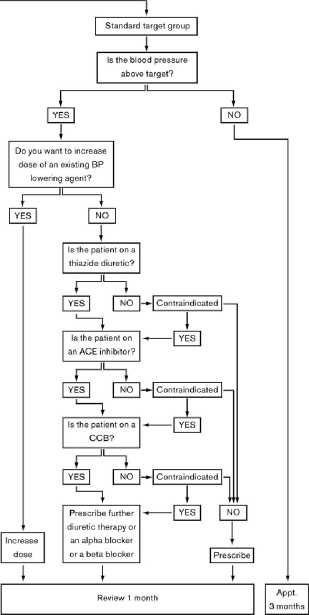
Figure 1 Summary of Algorithm for BP control.
supplied and validated for the study. The patient will be
seated for 5 minutes and then 6 measurements will be
taken at minute intervals. The second and third mea-
surements are averaged to give the reading. As the
intensive target group have their BP monitored more
frequently than those in the standard group, there may
be some diminution of the ‘white coat’ effect in this
group; the mean of readings 2 to 6 and the mean of 5
and 6 will be used to monitor for this. Any differences
between the groups in the primary outcome should be
sustained in the mean of the 5th and 6th readings (by
which time any accommodation effect is likely to have
worn off), enabling us to determine whether accommo-
dation has a significant effect in this study. 24 hour
blood pressure recordings using an ambulatory sphyg-
momanometer will be recorded at baseline and at twelve
months. 24 hour ambulatory measurement will be unaf-
fected by accommodation, so will provide further evi-
dence as to whether or not this was significant in this
study.
A variety of secondary outcome measures are also
assessed during the RN follow up appointments. (see
table 2) Key secondary outcomes are: additional
measures of BP (change in diastolic and mean daytime
ambulatory systolic BP between baseline and twelve
months); measures of adherence (including GP adher-
ence to protocol and patient adherence to prescribed
medication); quality of life (EQ5 D [19]; SF36 [20]); side
effects, tolerability and adverse events; clinical outcomes
(including major cardiovascular events [composite of
fatal and non-fatal stroke, myocardial infarction or fatal
coronary heart disease and other cardiovascular death],
all cause mortality, cognitive function [21] and hospital
admissions). Key secondary events (stroke; myocardial
infarction; fatal coronary heart disease and other cardio-
vascular death) will be reviewed by independent clini-
cians blinded to treatment to ensure unbiased coding of
these events.
Sample size
Randomisation of 610 patients (305 per arm), with 12
months of follow-up, will detect a 5 mmHg difference in
systolic BP between groups with 90% power and at a
significance level of 5% assuming a standard deviation of
17.5 mmHg (a conservative estimate of standard devia-
tion falling between 16, a figure derived from the same
sort of patients as included in this study [11] and 19,
More intriguing information
1. The name is absent2. Modelling the Effects of Public Support to Small Firms in the UK - Paradise Gained?
3. The name is absent
4. La mobilité de la main-d'œuvre en Europe : le rôle des caractéristiques individuelles et de l'hétérogénéité entre pays
5. The name is absent
6. THE AUTONOMOUS SYSTEMS LABORATORY
7. What should educational research do, and how should it do it? A response to “Will a clinical approach make educational research more relevant to practice” by Jacquelien Bulterman-Bos
8. Iconic memory or icon?
9. The name is absent
10. Word Sense Disambiguation by Web Mining for Word Co-occurrence Probabilities