Provided by Cognitive Sciences ePrint Archive
Online Journal of Health and Allied Sciences
Peer Reviewed, Open Access, Free Online Journal
Published Quarterly : Mangalore, South India : ISSN 0972-5997
Volume 9, Issue 4; Oct-Dec 2010

This work is licensed under a
Creative Commons Attribution-
No Derivative Works 2.5 India License
Case Report:
Olfactory Neuroblastoma: Diagnostic Difficulty
Vidya MN, Registrar, Department of Pathology, Apollo Hospitals, Bannerghatta Road, Bangalore 76
Swarna Shivakumar, Consultant Pathologist, Apollo Hospitals, Bannerghatta Road, Bangalore 76
Siddhartha Biswas, Consultant Pathologist, Apollo Hospitals, Bannerghatta Road, Bangalore 76
Vijay Shankar S, Associate professor, Department of Pathology, Adichunchangiri Institute of Medical Sciences, BG Nagara,
Nagamangala taluk, Mandya district, Karnataka
Address For Correspondence:
Dr. Vijay Shankar S,
No 45, Ananda shylam,
3rd cross, 1st main ,
KN extension, Yeswanthpur,
Bangalore - 560022,
Karnataka, India.
E-mail: [email protected]
Citation: Vidya MN, Shivakumar S, Biswas S, Vijay Shankar S. Olfactory Neuroblastoma: Diagnostic Difficulty. Online J Health
Allied Scs. 2010;9(4):18
URL: http://www.ojhas.org/issue36/2010-4-18.htm
Open Access Archives: http://cogprints.org/view/subjects/OJHAS.html and http://openmed.nic.in/view/subjects/ojhas.html
Submitted: Dec 6, 2010; Accepted: Dec 28, 2010; Published: Jan 20, 2011
Abstract:
Olfactory neuroblastoma is an uncommon malignant tumor of
sinonasal tract arising from the olfactory neuro epithelium. The
olfactory neuroblastomas presenting with divergent
histomorphologies like, epithelial appearance of cells, lacking
a neuro fibrillary background and absence of rosettes are
difficult to diagnose. Such cases require
immunohistochemistry to establish the diagnosis. We describe
the clinical features, pathological and immunohistochemical
findings of grade IV Olfactory neuroblastoma in a 57 year old
man
Key Words: Olfactory neuroblastoma; Nasal cavity;
Immunohistochemistry
Introduction:
Olfactory neuroblastoma is an uncommon malignant neoplasm,
representing 2-3% of sinonasal tract malignancies. It is a
malignant neuro ectodermal neoplasm arising from the
olfactory neuro epithelium found in the upper 1/3 to 1/2 of the
nasal septum, the cribriform plate and the superior medial
surface of the superior turbinate.1 This tumor has a broad
histological spectrum and olfactory neuroblastoma can be
confused with other small round cell tumors and
undifferentiated carcinomas. The diagnosis becomes difficult
when the cells have an epithelial appearance with scant or
absent neurofibrillary background. Immunohistochemistry is of
great value in differentiating ONB from other sinonasal tract
malignancies.
Case Report:
Left nasal polyp biopsy of a 57 year old male patient with 3
year history of left sided nasal obstruction was received in the
department of pathology. The patient presented with anosmia,
headache and loss vision in the left eye with worsening of
symptoms over the last 3 months. CT scan revealed a left
paranasal sinus lesion occupying the left maxillary, ethmoidal
region with intraorbital and intracranial extensions. MRI re-
vealed a left nasal mass extending and eroding the olfactory
groove at the anterior base with erosion of the left orbital wall.
Biopsy was done and sent for histopathological examination.
Gross Features: Multiple irregular grey white soft tissue bits
were received with a large polypoidal bit measuring 3x1.5x1
cm. Cut section was grey white with hemorrhagic areas.
Microscopy: Microscopic examination showed an intact respir-
atory mucosa with a tumor in the submucosa. The tumor cells
were seen predominantly arranged in large lobules, separated
by fibrovascular stroma with few areas of solid nests, cribri-
form pattern and comedo necrosis.(Fig.1) Occasional tumor
lobules showed Homer - Wright rosettes (Fig 2)
The cells were small to intermediate sized having vesicular
nucleus with single nucleolus and scanty to moderate amount of
acidophilic cytoplasm (Fig 3). Atypical mitosis of 2-3/10 HPF
was noted. No neuro fibrillary background was seen. The
stroma showed extensive areas of haemorrhage with mild
lymphocytic infiltration.
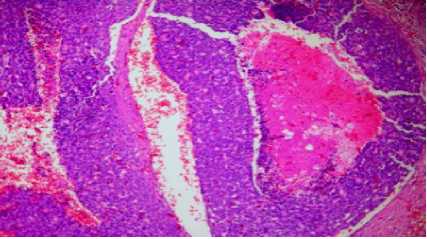
Figure 1: Photomicrograph showing tumor cells in lobules
with comedo necrosis (H&E X 100)