thoractomy being the second best outcome. Turning to look at the CT positive patients, we see
that the CWU strategy was actually more cost effective than the PET strategy with an ICER of
$A 24,484 per QALY. It is not possible to compare this with the NICE results because they did
not look at the CT positive patients as they believed this would not be a cost effective outcome
for PET as the model here shows.
Probabilistic sensitivity analysis
The role of probabilistic modelling is to further reflect the uncertainty in the parameters
used in the decision model and to see what effect this has, in this case, over the incremental net
benefit.47 The parameters in the model were given distributions with probabilities and utilities
given a beta distribution and all other costs and life expectancy given a gamma distribution. A
simulation was then run 10,000 times using the macro given in appendix 4.
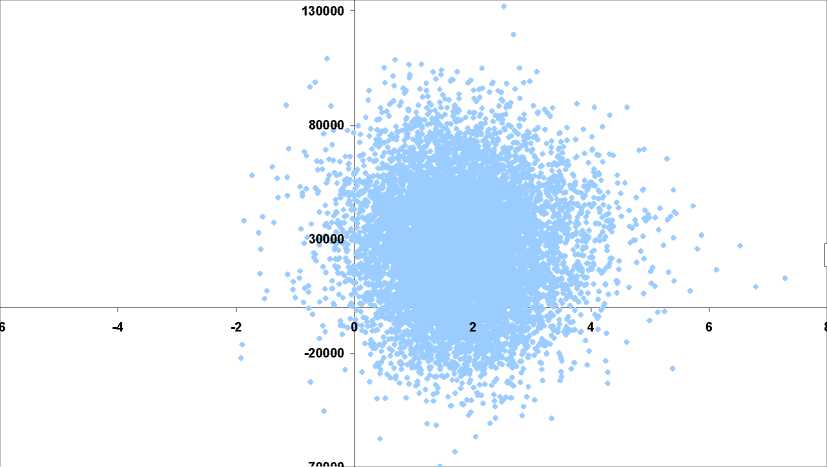
The graph below shows the following distribution of QALYS and costs and their
subsequent ICERs from the 10,000 simulation runs for the CT negative patients. It is clear that
the distribution is primary located in the more costly and more effective section of the graph
with a tight distribution of point with few extreme values. The current willingness to pay for
one QALY is not known and so the existing threshold ratio has not been added, but it clearly
shows that the threshold ratio would not have to be that high for the PET strategy to be
implemented.
Graph 1: The distribution of costs and QALYs and the resulting ICERs for CT negative
patients
ICERs
-70000
Incremental QALYs
<
v>
W
^ω
О
О
га
с
ф
E
ф
и
C
The next graph shows the distribution of ICERs in the 10,000 simulation runs for CT
positive patients. The distribution is also mostly located in the more effective and more costly
quadrant of the cost effectiveness plane. However the majority QALYs are located in a narrow
47 Briggs A., Claxton K. and Sculpher MJ. Decision analytic modelling for the evaluation of health technologies.
O.U.P., Oxford, 2006. p77
25
More intriguing information
1. THE UNCERTAIN FUTURE OF THE MEXICAN MARKET FOR U.S. COTTON: IMPACT OF THE ELIMINATION OF TEXTILE AND CLOTHING QUOTAS2. The name is absent
3. The name is absent
4. Cross-Country Evidence on the Link between the Level of Infrastructure and Capital Inflows
5. he Effect of Phosphorylation on the Electron Capture Dissociation of Peptide Ions
6. Output Effects of Agri-environmental Programs of the EU
7. ¿Por qué se privatizan servicios en los municipios (pequeños)? Evidencia empírica sobre residuos sólidos y agua.
8. An Empirical Analysis of the Curvature Factor of the Term Structure of Interest Rates
9. The name is absent
10. The name is absent