Abstract:
Free peritoneal perforation is a rare complication of
Crohn's disease with a report of only 100 cases in the
literature. It needs an emergency exploration and an
unaware general surgeon is confounded in
intraoperative decision-making. We present our
experience when this rarity struck us in a district
hospital and briefly review the guidelines of optimal
management of this complication of Crohn's disease.
Key Words: Free perforation, Crohn's disease, Ileal
perforation
Case Report:
A 19-year old girl was referred to our hospital for
management of acute abdomen. She had a history of
colicky pain abdomen with distension and vomiting for
four months. All these complaints became more severe
for the past 3 days. Vomiting was bilious and associated
with decreased urine output. Her past and personal
histories were not contributory. Family history was
positive for tuberculosis. On examination, she was
malnourished, dehydrated and pale. BP was 100/70 and
pulse rate was 110 per minute. Abdomen was
distended and warm with loss of bowel sounds.
An erect x-ray abdomen was taken which showed gas
under diaphragm with dilated bowel loops. She under-
went exploratory laparotomy under general anesthesia.
Peritoneal fluid was feculent. Entire length of the bowel
was inspected and findings accurately recorded. Multi-
ple strictures and 3 perforations (Figure 1 and Figure 2)
were present in the distal ileum all within 60 cm from
ileocecal junction. Ileal mesentery was thick and friable
with no palpable adenopathy. Large bowel and rest of
the small bowel was grossly normal. Around 70 cm of
ileum was resected and a hand-sewn ileo-ileal anasto-
mosis was performed in two layers. Patient had an un-
eventful postoperative recovery.
OnlineJimnnifoj''}fenftfi ainfjAffi&í',5⅛wβF
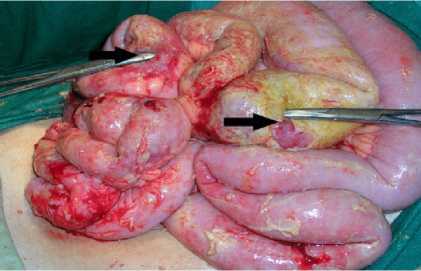
Fig. 1: Perforations in the terminal ileum (arrows)
Histopathological examination of the resected ileum
showed Crohn's disease. After postoperative recov-
ery, the medical gastroenterology department was
involved in her care. Immunosuppression (6-Mer-
captopurine, 1.5mg/kg) was started. The patient is
currently on follow-up with no clinical evidence of
disease recurrence.

Fig. 2: Stricture (arrowhead) and perforations
(arrows) in the terminal ileum
Discussion:
Crohn’s disease (CD) is a chronic relapsing and
remitting inflammation of the bowel involving all its
layers and characterized by noncaseating
granulomas. It has an unpredictable course and
surgical management is challenging. Majority of
patients with CD require surgery as time progresses,
such that 78% and 90% undergo surgery after 20
years and 30 years of symptoms, respectively.(1) The
most common indication for surgery in case of small
bowel CD is obstruction due to a terminal ileal
stricture while perforation, fistulae and abscess
formation account for the remaining. The
indications for surgery in Crohn's colitis include
abscesses (25%), perianal disease (23%), failure to
thrive (21%), toxic megacolon (19%) and intestinal
obstruction (12%).(2) Failure of medical
management in the form of persisting symptoms
despite aggressive therapy, recurring symptoms on
tapering and worsening symptoms during therapy is
another indication for surgical intervention.
Though contained ileal perforation with septic fea-
tures and inflammatory abdominal mass is common,
free perforation into the peritoneal cavity with gen-
eralized peritonitis is a rare presenting feature of
Crohn's disease with an incidence of 1-3% in West-
ern countries.(3) Only 100 cases have been reported
in literature.(4) In patients with intra-abdominal sep-
OJHAS Vol 6 Issue 4(6) Bhat MS, Ashfaque M, Balu K, Madhusudhanan J, Sendhil RK. A Rare Presentation of Crohn's Disease.

http://ojhas.org
More intriguing information
1. The name is absent2. The name is absent
3. Opciones de política económica en el Perú 2011-2015
4. Activation of s28-dependent transcription in Escherichia coli by the cyclic AMP receptor protein requires an unusual promoter organization
5. European Integration: Some stylised facts
6. Experimental Evidence of Risk Aversion in Consumer Markets: The Case of Beef Tenderness
7. Performance - Complexity Comparison of Receivers for a LTE MIMO–OFDM System
8. The name is absent
9. Achieving the MDGs – A Note
10. A parametric approach to the estimation of cointegration vectors in panel data